COMMENTARY: Masks-for-all for COVID *is* based on sound data
Drs. Brosseau and Sietsema,
This is an open-letter response to this article:
I found that your article to be inaccurate in several ways, and I wanted to offer some suggestions for corrections.
In your article, you argue that the #masksforall movement is based on unsound data and bad science. However, it appears that you have misinterpreted many of the studies that you cite, and have also simply overlooked many studies which show protective effects from mask wearing by the general public. I offer this open letter so that the public record may be corrected.
Prior experience mitigating SARS
In this first example, you appear to simultaneously misinterpret and ignore the same study. You mention Jefferson et al (2007) in the context of N95 masks not having superior efficacy to surgical masks, but the paper itself does not support that claim. It also appears to directly contradict the central thesis of your article:
The highest quality cluster randomised trials suggest that the spread of respiratory viruses into the community can be prevented by intervening with hygienic measures aimed at younger children. Meta-analysis of six case-control studies suggests that physical measures are highly effective in preventing the spread of SARS: … wearing masks (0.32, 0.25 to 0.40; NNT=6, 4.54 to 8.03); wearing N95 masks (0.09, 0.03 to 0.30; NNT=3, 2.37 to 4.06); …
This article argues that mask wearing in the community was 68% protective against SARS-CoV-1. This is in contradiction with your article’s title, as it indicates that #masksforall (at least surgical masks) are effective and based on sound data.
And as a side note, this article shows that N95 masks has a 91% protective effect vs the 68% effect for surgical masks. The confidence intervals for N95 and surgical masks do overlap slightly, so it’s not clear whether a direct comparison between the two would reach statistical significance. Overlapping CIs is not equivalent to a direct statistical test. At the very least, this would indicate a trend which these studies simply did not have enough statistical power to discern. At most, this would have been a significant effect if a proper statistical test had been performed. This is contrary to the assertion you were making when you cited that article.
RCTs on household use of face masks to protect against influenza
Results from RCTs appear to show that masks are protective when given to medical workers, but ineffective when given to community members. One plausible explanation for this is that medical workers get their masks fit tested, whereas community members do not. Another explanation is that community members usually use surgical masks, instead of N95s. However, there’s a third explanation which is obvious in retrospect but not apparent unless you read the literature very carefully.
Your article makes no mention of MacIntyre (2009), which is a particularly important article for two reasons. First, it shows that mask wearing by community members (parents of sick children) is 60–80% effective at protecting against influenza infection. Second, it shows why the majority of the other RCTs on face masks with influenza in the community have failed to show a similar effect. You see, MacIntyre (2009) had a null result in their primary intent-to-treat analysis. When they looked at whether giving masks to the parents and instructing them in the use of masks had protective effects, they found no significant effect. But they also did something that only two other studies I know of have done: they checked in afterward to see how many parents actually wore the masks. Very few, it turns out. Only 21% of household contacts in the intervention group reported wearing masks often or always. This makes it unsurprising that in the intent-to-treat analysis, no significant effect was found. But in their secondary analysis on the effect of adherence, they found masks to be 74% protective (95% CI, 23–91%), and that effect was no different between surgical masks and non-fit-tested P2 masks.
The problem isn’t that community members are wearing masks without fit-testing, or wearing ineffective masks. The problem is that community members generally don’t wear the masks when the threat is merely influenza.
A second study (Cowling et al, 2009) that examined adherence with influenza also found it to be low — 49% for patients and 26% for their parents. They found a protective effect of handwashing plus masks if the intervention was applied in the first 36 hours.
A third study (Suess et al 2011) found higher adherence — roughly 60%. That may have been due to a more thorough intervention in that trial: “Furthermore, we noted substantially increasing adherence after participants had received detailed instructions during a first household visit (Figs 1 and 2).” This implies that in order to get good adherence to the protocol, you have to check in on the families and remind them to use masks. Most studies didn’t do this, and are likely to show low adherence, similar to Cowling et al (2009). In addition to high adherence, this study also found masks to be effective (OR 0.30, 95% CI 0.1–0.94), again as long as they were deployed in the first 36 hours of the illness.
Of the six other RCTs discussed by MacIntyre (2015), none examined adherence or separately examined the effect of early vs late interventions. As they did not check on adherence, it is likely that they did not benefit from the effect found by Suess et all (2011), and adherence was probably low. These six RCTs together can be taken to imply that giving masks to people facing influenza is ineffective, but they do not imply that wearing masks is ineffective, as it is unlikely that many of the participants wore the masks.
Low adherence is not a problem in pandemic situations. During SARS-1, mask use by the community was 76%.
Fit
Your article argues that proper fit testing is key for good mask performance. The article implies, but does not explicitly state, that non-fit-tested masks are ineffective. This is not supported by the studies you cite. Those studies all compare fit-tested masks to non-fit-tested masks, and generally show fit testing to slightly improve protection. None of those studies include a no-mask group.
This is unsurprising; it is profoundly unethical to forbid medical workers from using PPE in cases of known exposure. This would be like asking skydivers to jump without a parachute. The only RCTs that can be done on PPE are either comparing one presumed-effective treatment to another, or testing PPE in situations where it isn’t actually necessary. This is a systematic problem with RCTs, and is the reason why the only RCT ever performed on the effectiveness of parachutes in preventing death found them to be completely ineffective. Ethical constraints limited skydiving jumps in that RCT to an altitude of 0.6 m.
Later, you also state the following:
A recent pooled analysis of two earlier trials comparing medical masks and N95 filtering facepiece respirators with controls (no protection) found that healthcare workers continuously wearing N95 FFRs were 54% less likely to experience respiratory viral infections than controls (P = 0.03), while those wearing medical masks were only 12% less likely than controls (P = 0.48; result is not significantly different from zero).
You assert that the control group was no protection, but this is incorrect. That kind of study would be unethical and can’t be performed, as mentioned above. Actually, that study’s control group was no change from standard practice, which included some unspecified degree of mask wearing. The researchers said that the hospitals used for the control arm were selected because they had “low levels of routine mask use,” but they did not elaborate, and did not measure or report those mask use rates. I interpret that to mean that these doctors and nurses used surgical masks or N95 masks for high-risk procedures but were barefaced at other times. With this interpretation, the study would only show that wearing surgical masks during low-risk procedures confers no significant benefit.
Hubei, South Korea, masks, and COVID
Early on in the article, you imply that mask use in Hubei prior to COVID failed to prevent the spread of the disease, and that this indicates that masks are ineffective:
Sweeping mask recommendations — as many have proposed — will not reduce SARS-CoV-2 transmission, as evidenced by the widespread practice of wearing such masks in Hubei province, China, before and during its mass COVID-19 transmission experience earlier this year.
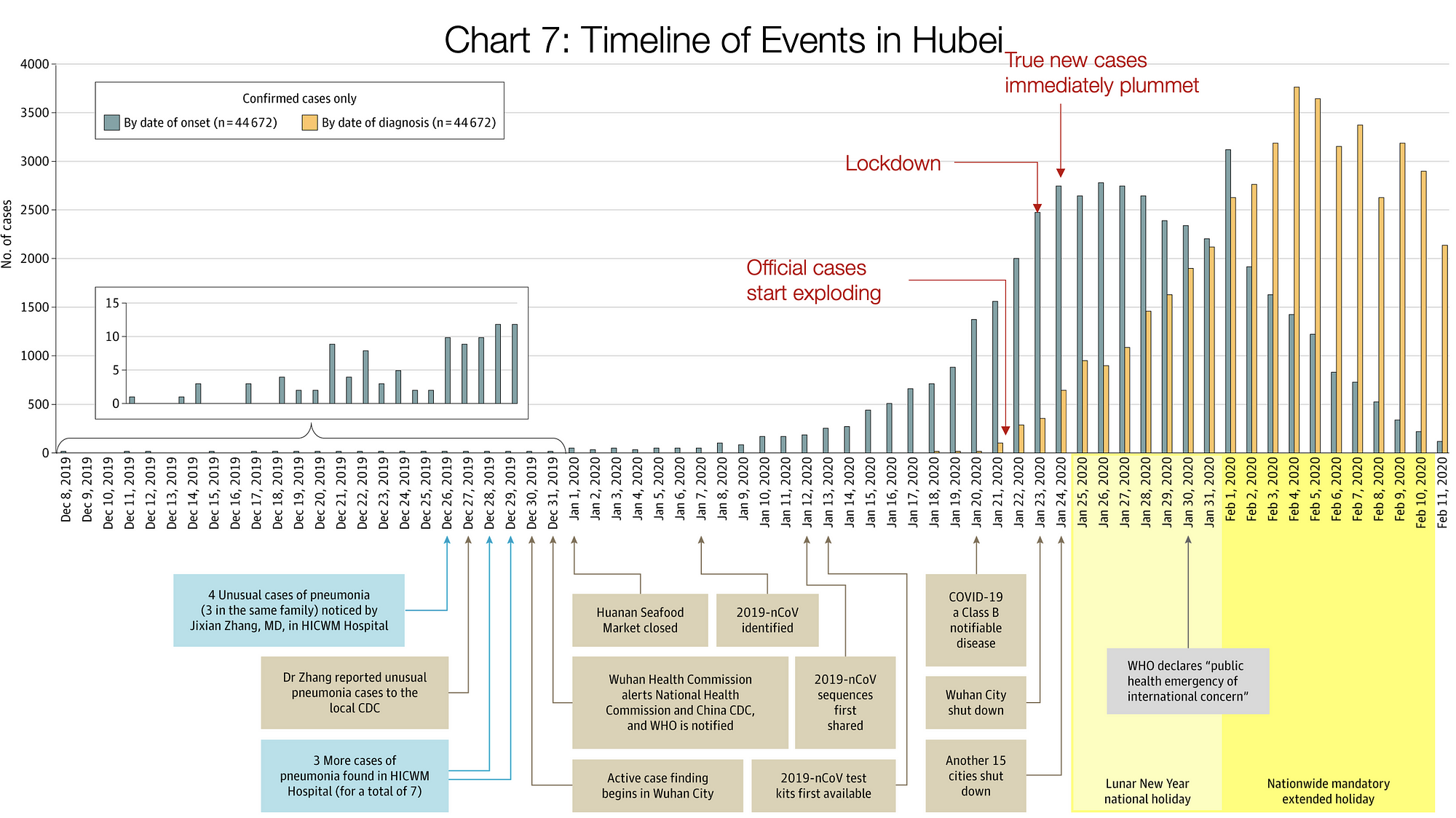
However, this statement is factually inaccurate: mask use in Hubei was extremely low prior to COVID and during the initial stages of the outbreak. You can see this by checking youtube for videos taken while walking around downtown Wuhan. This one from December 2019 is particularly informative. Of the first 43 people I saw in that video, not one was wearing a mask. (I did not watch the whole thing.) In contrast, this Jan 26, 2020 video shows exactly the opposite — not one person in the entire video was maskless outside. This is consistent with the timeline of political events in Wuhan. On Jan 15th, the Chinese government was still downplaying the severity of the outbreak. They made an abrupt about-face a week later, and on Jan 22nd they instituted lockdown in Hubei and made the use of facemasks mandatory nationwide, and the police began punishing anyone who went out without them. The incubation period of COVID can be as long as two weeks. Two weeks after universal facemasks and lockdown were instituted, the number of new cases in Hubei plummeted. This is hardly proof that masks were responsible, but it is fully consistent with the hypothesis that masks were helpful, and inconsistent with your assertion.
{kind=link}
A more suggestive example is South Korea. South Korea made near-universal use of masks, but did not institute a lockdown, and were nonetheless successful in containing and ending a large-scale outbreak. South Korea’s general public’s behavior on masks shifted dramatically as a result of the outbreak. In February, 2020, a survey was conducted of mask use in Korea. Only 19% of Koreans reported wearing face masks before COVID, but 89% reported doing so after COVID. This video of Seoul’s streets on March 14th corroborates those numbers.
Hong Kong is another interesting example. According to this video from March 16th, mask usage in Hong Kong appears to be >95%. Hong Kong has so far been able to suppress the virus and avoid a major outbreak, despite many early cases coming from Hubei. They have not instituted a lockdown or curfew, though they did close schools and eliminate public gatherings (e.g. no more protests).
Japan also is an informative example. Mask use in Japan is high, but not universal. In this March 21st video from Tokyo, mask use in Japan appears to be roughly 50%. At the same time, Japan has not been able to contain the virus, but has seen much slower spread than Western countries or early Wuhan, with a caseload doubling every 10 days in Japan compared to every 2.5 days for the USA. This observation is once again consistent with the hypothesis that transmission is negatively correlated with mask use. Testing rates are low in Japan, and social distancing practices are minimal. People are still going to work, and Tokyo’s streets are as packed as ever. The only alternate hypotheses I can think of for why Japan’s epidemic growth rates are so low is Japan’s culture of cleanliness and low-touch interpersonal interactions.
Italy is an interesting example because it appears to disprove the hypothesis that lockdown alone is a sufficient explanation for the reduction in cases in Wuhan. Italy instituted a nationwide lockdown on March 9th. If Wuhan’s example were representative, then we would expect to see cases begin to decline 14 days later. However, unlike China and South Korea, the rate of new cases in Italy never declined; it stabilized around March 21 at ~4000 new cases per day and remained at that level since. Mask usage by the general public in Italy is low among HCWs as well as the general public, due to the shortage.
Conclusion
Yes, there is a shortage of masks and respirators, and it’s important that they be allocated first where they will do the most good, as per the principles of triage. Yes, the data on the efficacy of cloth masks is weak, and cloth masks probably have only a small effect. But surgical masks appear to be quite effective when worn by the general public, and universal surgical mask use may be enough to halt this pandemic entirely, even after lockdown has been lifted.
We should be treating this shortage as a supply-side problem, not a demand-side problem. If we tell people that masks don’t work, we’ll end up doing a lot of damage that we can’t undo later after the supply-side problem is resolved. Adherence is typically the most difficult problem to overcome with mask use, and telling people now that they don’t work is likely to be a mistake.
I hope this commentary on your commentary has been helpful.
Jonathan Toomim
(BA, Molecular & Cellular Biology, UC Berkeley)